The Optimisation Problem: What Bryan Johnson’s 5-MeO-DMT Experiment Reveals About Psychedelics Going Mainstream
This is a Guest Article by Ryan Khan. Any views are his own and do not necessarily reflect those of Psychedelic Alpha or its team.
A 27 mg dose, a delayed protocol, and the risks of translating psychedelics into an optimisation framework.
On March 22nd, tech centimillionaire and biohacking entrepreneur Bryan Johnson livestreamed himself taking 27 mg of 5-MeO-DMT. It was his second public psychedelic experiment, part of his ongoing Blueprint program and broader mission to push the limits of human longevity. But beyond the spectacle, the livestream raises a more structural question: What happens when a highly variable, difficult-to-standardise psychedelic experience is translated into an optimisation framework and broadcast to millions?
Bryan Johnson, founder of Kernel, made his fortune after selling Braintree for $800 million in 2013. He is now known for his extreme, highly quantified—and at times theatrical—approach to slowing aging, often summarised in his “Don’t Die” mantra. The effort reportedly costs around $2 million annually and has included blood transfusions from his son, follistatin gene therapies, and more than 100 daily supplements—all in pursuit of reversing his biological clock.
Psychedelics have recently been incorporated into this framework. In 2025, Johnson conducted two high-dose psilocybin sessions within a three-week period, culminating in a livestreamed experiment with 5.35 g of dried Psilocybe cubensis (~28 mg psilocybin) at a licensed facility in Oregon on November 30th. The 5.5-hour broadcast was framed as the “most quantified psychedelic experiment” to date, tracking 249 biomarkers across the experience.
Following what he described as “compelling” longevity signals (n=1), Johnson has begun positioning psychedelics not just as therapeutic tools, but as components within a broader optimisation strategy targeting multiple physiological systems.
The 5-MeO-DMT session marks a clear escalation—both in intensity and implication.
Inside Johnson’s 5-MeO-DMT experiment
In his latest experiment, Johnson set out to test whether a single high-intensity 5-MeO-DMT session could measurably influence biological markers associated with aging.
Across a 2.5-hour livestream, his team tracked physiological and neurological signals using MRI, fMRI, EEG, and other biomarker monitoring tools. The broadcast drew 249,000 live viewers and has since received 1.5 million views on X, becoming one of the most widely viewed pieces of psychedelic dosing content ever.
The session took place in a controlled indoor setting on Bowen Island, British Columbia, a region where underground psychedelic practice continues to operate alongside formal research and grey-market pathways. Johnson was joined by his partner and son, alongside facilitator and Enfold Institute co-founder Steve Rio, who prepared and administered the 5-MeO-DMT doses. Music was streamed live by handpan artist Malte Marten, introducing a ceremonial layer into an otherwise clinically oriented environment.
Shortly before dosing, Bryan Johnson spoke with Robin Carhart-Harris, who described 5-MeO-DMT as the “god molecule”, the “Everest of psychedelics”, and among the most intense altered states reported.
This framing draws on the idea that high-dose psychedelic states transiently relax hierarchical brain dynamics, increasing neural flexibility and disrupting entrenched patterns of cognition—an interpretation consistent with the REBUS and entropic brain models, though its extension to aging biology remains speculative.
Pharmacologically, 5-methoxy-N,N-dimethyltryptamine (5-MeO-DMT) acts as a nonselective serotonin receptor agonist, with a 300–1000-fold higher affinity for 5-HT1A relative to 5-HT2A receptors. This profile is often used to explain its distinct phenomenology: rapid ego dissolution with comparatively limited visual content relative to classical psychedelics. Consistent with this, it has been described as inducing a “global mode of deconstructed consciousness”.
“These kinds of experiences can wipe away … the ways of understanding the world … leading to not knowing what’s real anymore”, Timmy Davis, Director of the Centre for Evidence-Based Drug Policy and founder of The Psychedelic Experience Clinic, noted during a recent panel discussion hosted by The Psychedelic Society. “When people are exposed to these modes of ego death or controlled traumas”, he adds, “it’s vitally important they’re taken good care of after, and that the setting is tightly controlled.”
The dose: 27 mg in context
A total dose of 27 mg places Johnson’s session at the extreme upper end of contemporary 5-MeO-DMT use. What that represents in practice depends on context, spanning clinical trials, structured retreat settings, and emerging underground protocols.
In clinical research, dosing strategies typically favour controlled escalation or more moderate doses. For example, GH Research employs an individualised regimen for inhaled 5-MeO-DMT (GH001), administering up to three escalating doses (6 mg, 12 mg, 18 mg) within a single session if a predefined “peak experience” is not achieved. In a Phase 2b trial in treatment-resistant depression (TRD) (n=81), this approach produced rapid antidepressant effects, with a 15.5-point reduction in MADRS scores at Day 8 and 57.5% remission.
Similarly, AtaiBeckley’s intranasal candidate (BPL-003) has shown efficacy at more modest doses. In a Phase 2b trial in TRD (n=193), single 8 mg and 12 mg doses produced rapid and clinically meaningful reductions in depression severity, with effects emerging by Day 2, deepening by Day 8, and sustained through at least Day 57. The programme has received FDA Breakthrough Therapy designation and is advancing toward Phase 3 this quarter, with 8 mg as the lead dose.
Taken together, these models reflect a broader clinical trend: prioritising reliability and tolerability at lower or titrated doses, rather than using maximal intensity as a proxy for therapeutic effect.
Outside regulated trials, practices are more heterogeneous but still emphasise structure over intensity. Retreat settings such as Tandava involve multi-day programmes with screening, preparation, and integration, often using multiple lower or moderate doses. Similarly, organisations like The Mission Within embed 5-MeO-DMT within broader treatment frameworks, adjusting dosing based on individual response and readiness.
“Dosage with this molecule is the most important … the quality of someone’s process [varies] based on accurate and appropriate dosing”, Otto Maier, Head of Integration at Tandava Retreats and founder of Soul & Psyche, said in the panel, emphasising that dosing protocols should be individual-specific. “The route of administration really matters … when Bryan says he did 27 mg, my first thought is that’s a lot of medicine”, he continues. “Dosage makes a huge difference, and so does the specificity of someone’s process.”
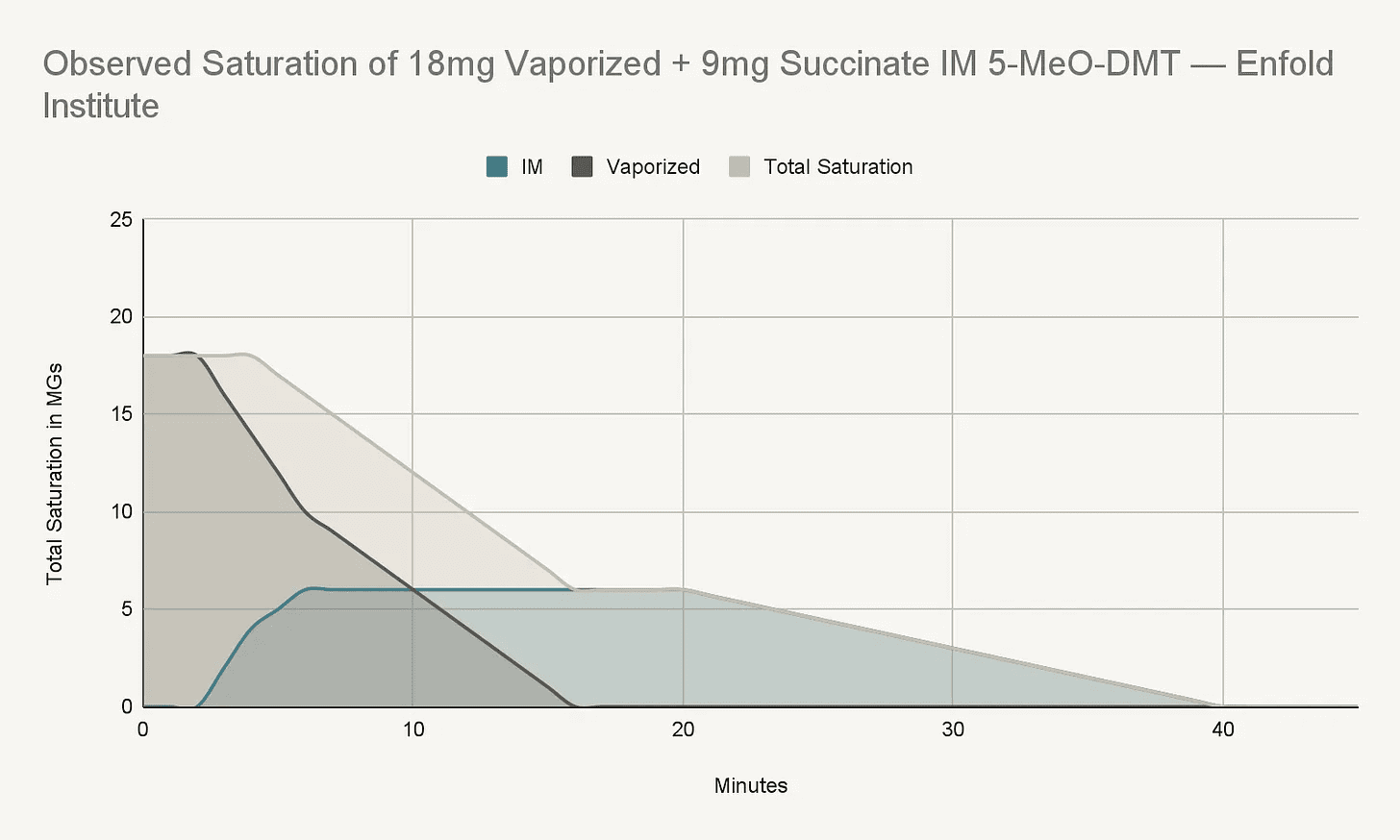
Johnson’s session, by contrast, followed a dual-route model later formalised by the Enfold Institute as the “Leckie Protocol”, combining a 9 mg intramuscular (IM) injection with 18 mg vaporised.
Pharmacologically, this combination shapes both onset and duration, engineering the dynamics of the session in a way neither route can achieve independently. Vaporised 5-MeO-DMT produces an almost immediate onset (5-7 seconds), driving rapid ego dissolution and somatic release, while the IM component (onset ~3-4 minutes) extends the experience into a longer plateau, potentially allowing greater therapeutic engagement.
“With 5-MeO-DMT, you go from nought to 10 in seconds, maybe minutes. The runway is really short … and that rapidly rising intensity can be very overwhelming”, Hattie Wells, co-director of Breaking Convention and research therapist on AtaiBeckley BLP-003 trials, explains in the panel. “You can have a flash of insight, but without ongoing support those insights can slip away”, she adds, “it’s about mitigating risk and sustaining outcomes through longer-term support.”
Within this model, the two routes act synergistically: a rapid breakthrough phase followed by a prolonged therapeutic window, potentially increasing retention of the experience compared to vaporisation alone.
The Leckie Protocol draws on observational data from more than 650 sessions and is reported to operate within a structured five-day therapeutic container. Dosing is individualised based on factors such as
sensitivity, prior experience, and psychological readiness, typically informed by a low-dose preparatory session the day before.
Much of this context, however, was absent from the livestream. While Johnson referenced a lower “trial” dose (2×1 mg and 2×1.5 mg vaporised 5 minutes apart, followed by 3 mg IM) the day before, the broader framework (including screening, preparation, and integration) was not meaningfully discussed. Critically, the full protocol was only released four days later.
As a result, millions of viewers have witnessed a high-dose intervention largely in isolation, lacking the safeguards that typically accompany it. Without that context, this risks framing the session as a standalone peak experience rather than a structured therapeutic process.
Even within the Leckie framework, where typical ranges sit around 6-9 mg IM and 10-18 mg vaporised, Johnson’s session sits at the upper boundary, intentionally stacking peak intensity with extended duration.
While comparable doses have been reported in naturalistic settings, including work by Chris Timmermann documenting sessions up to ~28.5 mg inhaled 5-MeO-DMT, such exposures remain rare, highly context-dependent, and accompanied by extensive safety considerations.
“While there is high variability in dose response, 27 mg is far beyond what most people take”, Hattie Wells says. “Alexander Shulgin indicated doses above 20 mg were a no-go, with a sweet spot around 10 mg … and in AtaiBeckley trials, optimal dosing now sits around 8 mg”, she adds, “so 27 mg is off the scale for most people.”
Across these models, a consistent pattern emerges: strong emphasis on screening, preparation, and structured dosing. Johnson’s approach reflects a different logic, more aligned with optimisation culture, where maximal input is assumed to produce maximal output.
With 5-MeO-DMT, however, the relationship between dose and outcome is not linear. Beyond a threshold, increasing intensity may not enhance therapeutic value, and may instead elevate risks such as reactivation, sleep disruption, and psychological dysregulation.
“The potential for acute psychological overwhelm increases the higher you go … you can lose your sense of self and develop confusion or paranoia because you’re not tethered to reality”, Anya Ragnhildstveit, Clinical Research Scientist and founder of Pneuma Science, who published the first paper assessing 5-MeO-DMT for PTSD, noted during the panel discussion. “It can impair your ability to manage yourself safely, especially without preparation, monitoring, and support”, she adds, “with risks spanning psychological and physiological domains, including reactivation events that can occur days, months, or even years later.”
What happens when millions are watching?
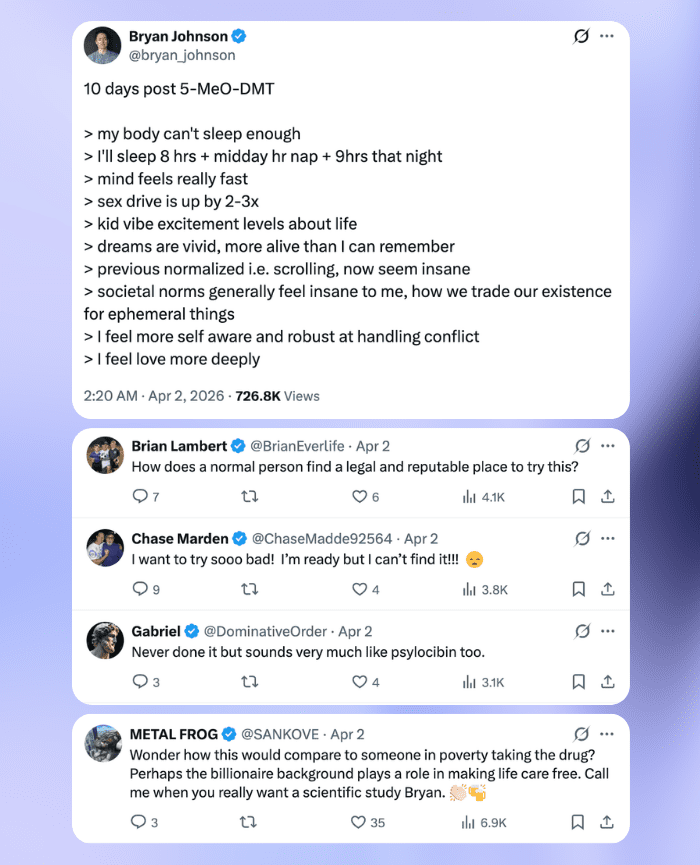
To be clear, Bryan Johnson is not explicitly encouraging replication. But influence in this context rarely operates through direct instruction. When an individual with his reach describes 5-MeO-DMT as “the most profound experience of my life” or “the ultimate prize”, it functions less as personal reflection and more as a signal—one that may be interpreted as something to explore or replicate.
A widely viewed, high-intensity session also establishes an implicit reference point for what constitutes a meaningful or complete 5-MeO-DMT experience, shifting attention toward method, structure, and expected outcome.
In psychedelics, this distinction is consequential. Set and setting are well-established determinants of both acute experience and longer-term outcomes, while expectations—particularly those shaped by highly visible narratives—can influence both phenomenology and integration.
“We’re seeing signals that expectancy can influence outcomes … whether you believe a psychedelic will help or not”, Anya Ragnhildstveit notes. “But we have a lot more to learn, there’s nothing definitive yet”, she adds, “what we do know is that beliefs are shaped by what people see and hear … from media, podcasts, and livestreams.”
From this perspective, large-scale exposure to a single narrative can therefore standardise preconceptions, orienting individuals toward specific experiential targets such as “breakthrough” or ego dissolution, while shifting attention away from variables like dose calibration, therapeutic support, and the broader contextual factors that shape both safety and outcome.
“What concerned me was that you didn’t see any of the preparation or integration—only the dosing, and a significantly high dose at that”, Hattie Wells says. “Johnson mentioned in passing that he took some the day before, but didn’t expand on it—what dose, how it was, who was with him”, she adds, “presumably different doses were tested to find his sweet spot, but none of that was explained.”
This dynamic is compounded by how Johnson’s session was presented. The dual-route approach, or Leckie Protocol, was shown to a mass audience before its full therapeutic context was available, leaving the dose and acute experience as the most salient elements.
More broadly, this raises questions about how psychedelic interventions are translated into public-facing formats. Increased visibility is not inherently problematic—in many respects, broader discussion is necessary as clinical development accelerates. However, the manner of presentation is critical.
5-MeO-DMT is not easily situated within optimisation frameworks: its effects are highly context-dependent and often among the most intense reported in human experience. Packaging such an intervention as a livestream, particularly when embedded within a performance narrative, risks flattening a complex, deeply subjective, multi-stage process into a simplified representation.
In this case, preparatory and integration processes remained largely implicit or were disclosed only after the broadcast, skewing attention toward the peak experience. For viewers without equivalent context or support, this superficiality alters the risk profile.
Standard disclaimers such as “Don’t try this at home” are unlikely to offset observational learning. In a highly visible and positively framed context, the combination of exposure, endorsement, and incomplete information may shape behaviour in ways that extend beyond Johnson’s intentions.
Can psychedelics really slow aging?
A central claim emerging from Bryan Johnson’s experiment is that psychedelics, particularly 5-MeO-DMT, may have relevance for longevity, with Johnson describing the compound as “one of the most underrated longevity tools” capable of “resetting” biological systems.
At present, this claim sits well ahead of the available evidence.
“There is no clinical evidence to support longevity claims at this point in time… the literature is still emerging”, Anya Ragnhildstveit comments. “In a livestream format, there is an obligation to educate the public”, she adds, “particularly given the differences between clinical, recreational, and underground use.”
There is growing interest in how psychedelics may interact with aging-related biology, including neuroplasticity, inflammation, and cellular resilience. A widely cited npj Aging study found that psilocybin and psilocin extended cellular lifespan in vitro and improved survival in aged mice. However, these findings were generated under controlled conditions using repeated high-dose administration (15 mg/kg), limiting their relevance to single-exposure human use.
Preclinical work suggests 5-MeO-DMT may promote neurogenesis, neuronal survival, and immunomodulatory effects. But there is currently no human evidence that it, or any psychedelic, can meaningfully slow or reverse aging. Translating these early signals into organism-level outcomes remains conjectural, even if mental health improvements may indirectly influence longevity.
Positioning 5-MeO-DMT as a longevity intervention shifts the conversation from exploratory science toward implied application, collapsing the distinction between early mechanistic findings, what Robin Carhart-Harris has described as “science in a sense”, and clinically validated outcomes. Within biohacking frameworks, this creates a mismatch: psychedelics may hold therapeutic potential, but they do not yet function as measurable anti-aging interventions. Framing them as such risks getting ahead of the science.
Looking forward
Johnson’s experiment sits at the intersection of several emerging trends: increasing psychedelic visibility, expanding clinical research, and optimisation-driven self-experimentation—each operating under a different logic. The livestream ultimately highlights the difficulty of translating between them.
5-MeO-DMT cannot be meaningfully separated from its context. Outcomes are shaped as much by preparation, setting, integration, and wider social matrixes as by dose or pharmacology. When these factors are minimised in public-facing narratives, what remains is an incomplete picture—one that privileges peak intensity over broader therapeutic process.
As visibility scales, this distortion becomes more consequential. For many viewers, the session will register less as a structured intervention and more as a standalone experience defined by dose and outcome. The later release of the Leckie Protocol adds context, but also underscores the asymmetry between what was shown and what was required to support it.
“Not focusing on the dosing experience so much, but the wider arc … the ‘matrix’ where people come from and where they return to”, Hattie Wells says. “Dosing is just one step along that arc … what your support network looks like before and after really matters”, she adds. “Neuroplasticity is not inherently good—the wider setting shapes how those pathways form.”
None of this negates the potential value of psychedelics, nor the importance of broader discourse. But it does point to a growing need for precision and clarity in how these experiences are communicated as they move into the mainstream.
“There was a sense the community needed to step in, given how quickly this could go south in terms of misinformation and harm”, Anya Ragnhildstveit says. “It was eye-opening to see how quickly people mobilised to educate the public about 5-MeO-DMT.”
As psychedelics enter wider cultural and commercial frameworks, the question is not only whether they work, but how they are understood, contextualised, and engaged with. In that sense, the challenge is not simply access, but interpretation. Ensuring that visibility does not outpace the structures needed to support safe and meaningful use may prove as important as the science itself.

Ryan Khan
Ryan Khan is a Research Assistant at Pneuma Science and an Events Coordinator for The Psychedelic Society, combining his expertise in psychedelic research, communications and community building. He is currently completing an MSc in Psychedelics at the University of Exeter.
Join thousands of psychedelics insiders
Get the weekly psychedelic medicine briefing.
A free weekly digest covering trials, regulation, policy, and access.
By signing up, you agree to our privacy policy. You can unsubscribe at any time.